Weight loss peptides comparison
in dept comparison of each o the 3 main weight loss peptides and how theyperform .
James
2/23/20262 min read
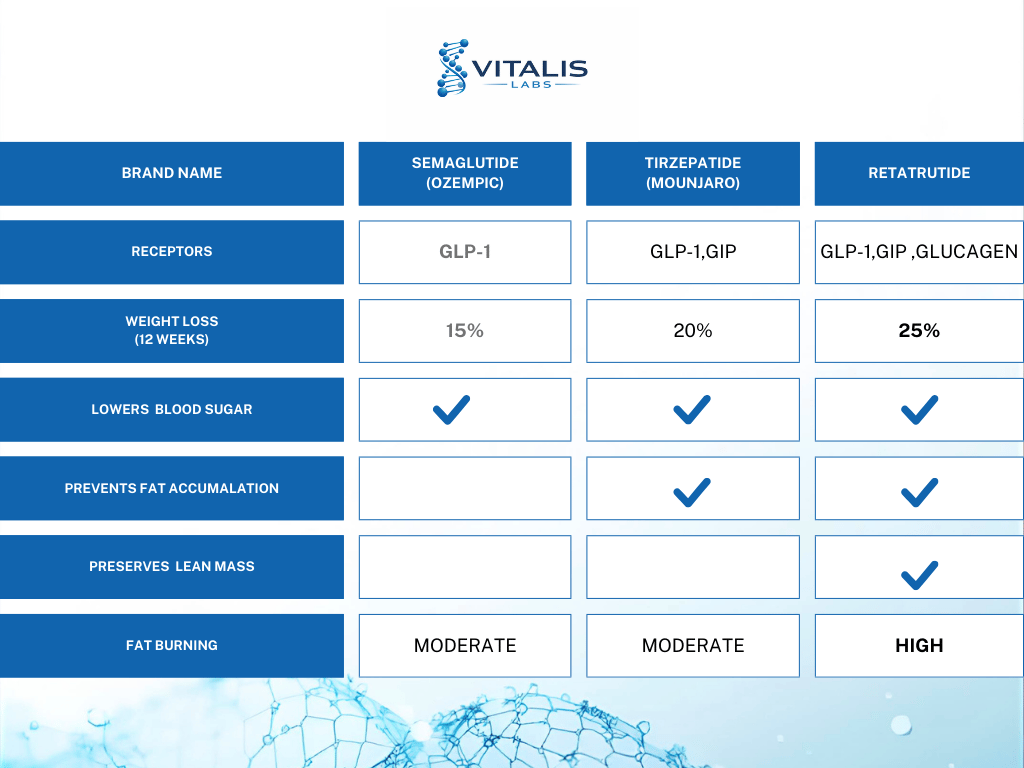
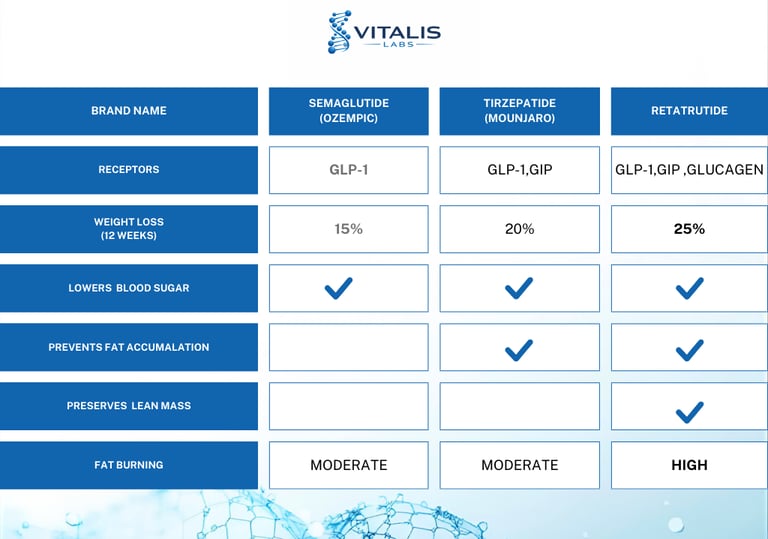
Retatrutide vs Tirzepatide vs Semaglutide: Mechanisms, Weight Loss Results, and Clinical Differences
Incretin-based therapies have transformed the treatment landscape for obesity and type 2 diabetes. Medications targeting GLP-1 pathways have demonstrated unprecedented weight loss outcomes, with newer multi-receptor agents pushing results even further.
This article provides a clinical comparison of:
Retatrutide (investigational triple agonist)
tirzepatide
semaglutide
We will examine mechanisms of action, clinical trial data, efficacy, tolerability, and future implications for obesity treatment.
Mechanism of Action: Single vs Dual vs Triple Agonism
Semaglutide: GLP-1 Receptor Agonist
Semaglutide selectively activates the GLP-1 (glucagon-like peptide-1) receptor.
Primary Effects:
Appetite suppression via hypothalamic signaling
Delayed gastric emptying
Increased glucose-dependent insulin secretion
Reduced postprandial glucose levels
Semaglutide targets appetite regulation primarily, making it highly effective for weight reduction and glycemic control.
Tirzepatide: Dual GIP + GLP-1 Agonist
Tirzepatide activates both:
GLP-1 receptors
GIP (glucose-dependent insulinotropic polypeptide) receptors
Added Benefits of GIP Activation:
Enhanced insulin sensitivity
Improved beta-cell function
Potential modulation of adipose tissue metabolism
Dual agonism enhances metabolic effects beyond GLP-1 alone, contributing to greater weight loss observed in trials.
Retatrutide: Triple GLP-1 + GIP + Glucagon Agonist
Retatrutide expands on this model by activating:
GLP-1 receptors
GIP receptors
Glucagon receptors
Unique Mechanism:
Appetite suppression (GLP-1)
Insulin sensitivity support (GIP)
Increased energy expenditure and fat oxidation (glucagon receptor activation)
The glucagon component may increase metabolic rate and lipolysis, potentially explaining the larger weight reductions seen in early trials.
Retatrutide is currently investigational and being developed by Eli Lilly and Company.
Weight Loss Comparison: Clinical Trial Data
Semaglutide (STEP Trials)
In obesity trials:
Average weight loss: ~15% of body weight
Significant improvements in HbA1c and cardiometabolic markers
Semaglutide marked a major breakthrough when first introduced for chronic weight management.
Tirzepatide (SURMOUNT Trials)
In adults with obesity:
Average weight loss: ~20–22% at higher doses
Significant waist circumference reduction
Improved insulin resistance markers
Tirzepatide demonstrated greater weight loss than GLP-1 monotherapy.
Retatrutide (Phase 2 Data)
In Phase 2 obesity trials:
Mean weight loss up to ~24% at 48 weeks (highest doses)
Continued downward weight trajectory at study endpoint
Favorable lipid and cardiometabolic improvements
Retatrutide’s results approach weight reductions historically seen with bariatric surgery in some participants.
Phase 3 trials are ongoing to confirm long-term safety and efficacy.
Glycemic Control Comparison
MedicationHbA1c ReductionMechanism StrengthSemaglutideStrongGLP-1 mediatedTirzepatideVery strongGLP-1 + GIP synergyRetatrutidePromising (early data)Triple pathway modulation
All three demonstrate glucose-lowering benefits, but tirzepatide and retatrutide may offer enhanced metabolic modulation due to multi-receptor activity.
Cardiometabolic Impact
Beyond weight loss, these medications influence:
Blood pressure
Lipid profiles
Liver fat content
Inflammatory markers
Semaglutide has demonstrated cardiovascular benefit in outcomes trials. Tirzepatide cardiovascular data is emerging. Retatrutide cardiovascular outcome trials are ongoing.
Which Is Most Effective for Weight Loss?
Based on available data:
Semaglutide: ~15% average weight loss
Tirzepatide: ~20–22% average weight loss
Retatrutide: Up to ~24% in early trials
Retatrutide currently shows the greatest average weight reduction, though it remains investigational.
The Future of Obesity Pharmacotherapy
The evolution from single to triple receptor agonism reflects a shift toward treating obesity as a complex, multifactorial metabolic disease rather than a purely behavioral issue.
Future directions may include:
Earlier pharmacologic intervention
Combination therapies
Personalized metabolic targeting
Expanded cardiovascular outcome research
Triple agonists like retatrutide may represent the next frontier in obesity medicine.
Conclusion
Semaglutide revolutionized medical weight management. Tirzepatide enhanced efficacy through dual incretin action. Retatrutide may further advance the field with triple-hormone receptor targeting that addresses appetite, insulin sensitivity, and energy expenditure simultaneously.
While semaglutide and tirzepatide are currently approved and widely used, retatrutide’s early data suggests it may become one of the most potent anti-obesity medications if Phase 3 trials confirm safety and efficacy.
As obesity treatment continues to evolve, multi-receptor peptide therapies are redefining what is possible in non-surgical weight management.